Workflow vs Agent: Cutting Through the AI Semantics
We are getting lost in the semantics of what an AI agent is versus just AI.
Let’s simplify it.
Start with what we all know: ChatGPT or any AI-powered app. It is an application driven by a large language model. You ask a question. It responds. Every interaction is initiated and directed by you, the human.
Even when we make these systems more useful by giving them “tools” through standards like Model Context Protocol, the interaction is still fundamentally prompt-driven. The human decides the goal. The AI executes within that scope.
If an AI app accesses a patient’s medication list or integrates with a scheduling system, that is powerful. But it is not necessarily agentic. It is still a workflow determined by the human prompt.
So what makes something truly agentic?
What Makes AI Agentic?
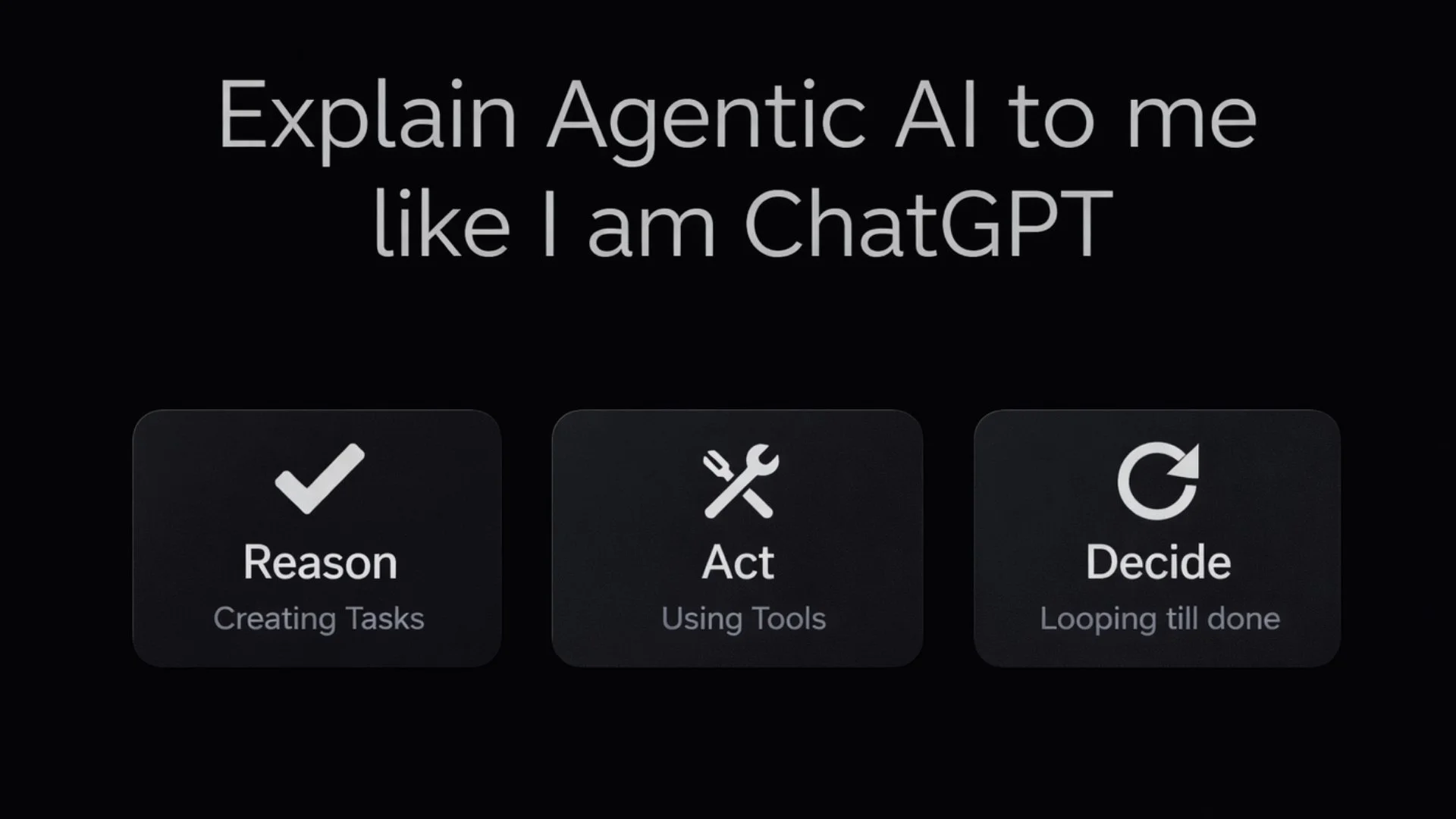
For an AI system to be genuinely agentic, it needs three capabilities: reason, act, and decide within an autonomous loop.
1. Reason
An agent must be able to reason about a goal and determine the best actions to achieve it.
For example, imagine giving the system the goal: “Optimize patient flow.”
A basic AI workflow would wait for a specific instruction, such as “Show me wait times.”
An agentic system would interpret the goal and decide what tasks are required. It might:
Analyze real-time wait times
Assess physician availability
Identify bottlenecks
Propose dynamic re-routing or rescheduling
The key difference is that the agent decides what tasks are necessary to achieve the objective.
2. Act
Once tasks are identified, the agent must be able to act.
This is where tools come into play. The agent may:
Query clinical guidelines
Send secure messages to patients
Update a patient’s chart
Trigger scheduling workflows
Generate documentation
Tools are necessary for agentic systems. However, simply using tools does not make a system agentic. The distinction lies in who determines when and why those tools are used. In an agentic system, that decision originates from the agent’s reasoning about a goal, not directly from a human instruction.
3. Decide: Orchestration and Iteration
The defining characteristic of agentic AI is the autonomous loop.
An agent acts, observes the result, evaluates progress toward the goal, and adjusts its approach. This iterative cycle continues until the objective is satisfied.
This decision-making loop often includes internal orchestration. For example:
One LLM drafts a personalized treatment plan.
A separate “critic” LLM evaluates it for guideline adherence and patient preferences.
If deficiencies are detected, the system revises and improves the plan before presenting it.
The agent is not simply responding. It is self-evaluating and refining without a human directing each step.
This continuous, self-correcting process, operating without a human in the decision-making loop, is the hallmark of true agentic AI.
Where Does Healthcare Stand Today?
Given this definition, it is unlikely that we will see widespread deployment of fully autonomous agentic AI in core clinical decision-making in the near term.
Administrative workflows are a more natural fit. Prior authorizations, scheduling, billing, and documentation automation are structured enough to support increasing autonomy.
Clinical decision-making is different. It demands contextual judgment, ethical oversight, and accountability that autonomous AI systems are not yet ready to assume independently.
What we will see, however, are increasingly powerful AI workflows. These systems will integrate advanced tool invocation, structured reasoning, guardrails, and human oversight. They will provide invaluable decision support and cognitive augmentation.
They may not be fully autonomous agents, but they will significantly elevate how care is delivered.
Semantics vs Impact
Ultimately, we should not become trapped in the semantics of “workflow” versus “agentic.”
Whether we label a system as an advanced workflow or an emerging agent, the more important question is this:
Does it improve efficiency?
Does it personalize care?
Does it augment human expertise responsibly?
Does it lead to better patient outcomes?
The focus should not be on terminology. It should be on building systems that leverage these capabilities safely and meaningfully.
The real transformation in healthcare will not come from what we call the system. It will come from how effectively we design, govern, and integrate it.