SMART on FHIR: We Built the App Store Rails. So Where’s the App Economy?
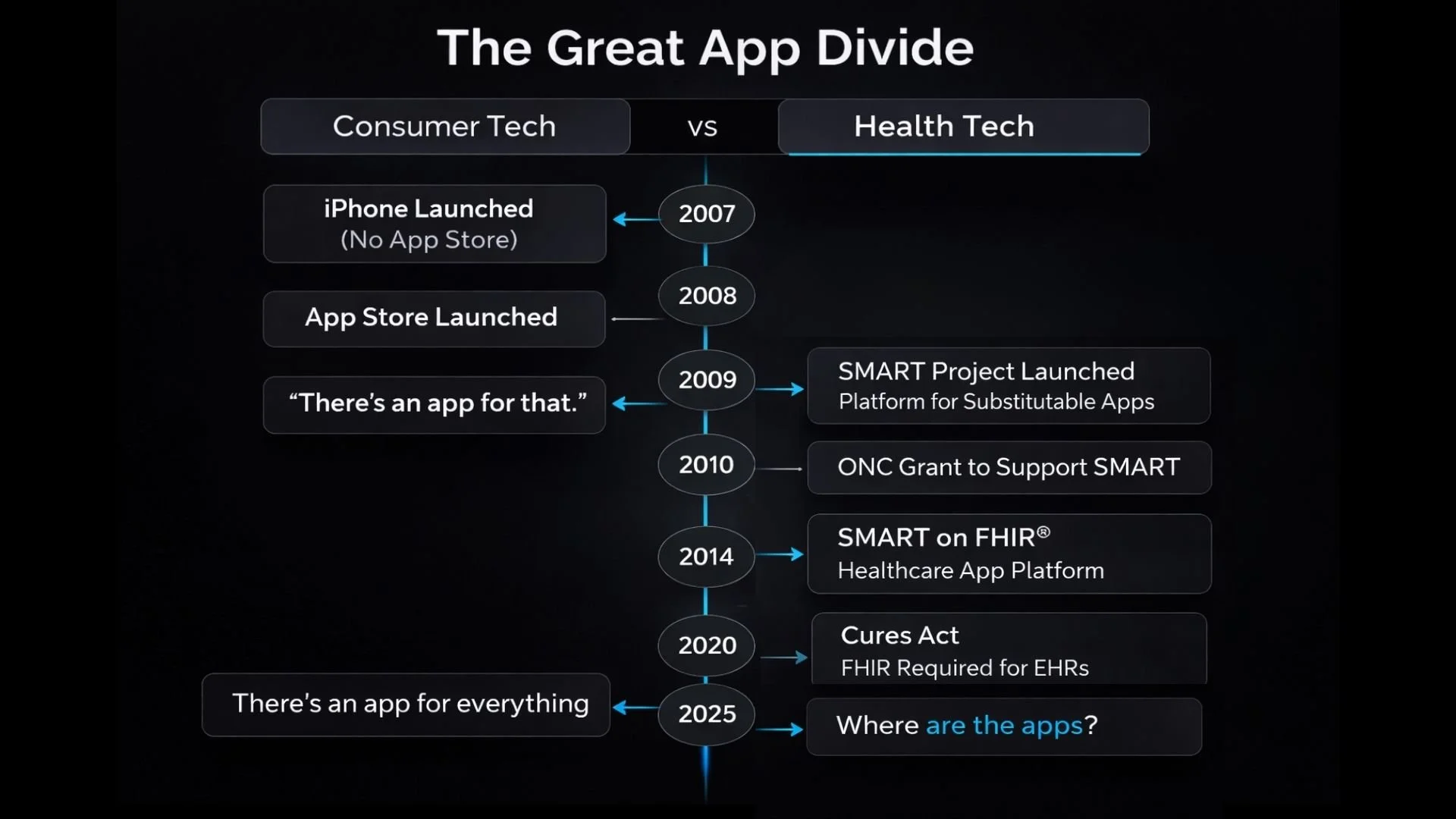
When the iPhone launched in 2007, Steve Jobs initially discouraged native third-party apps. Instead, he advocated for web apps accessed through Safari.
By 2008, Apple reversed course and launched the App Store. The rest is history.
An ecosystem was born. Developers built once. Apps ran everywhere. Substitutability drove innovation, competition, quality, and price transparency.
Healthcare had its own “App Store moment” vision.
The Audacious Goal
In 2009, the SMART project was launched. As outlined on the SMART Health IT website:
“The goal of the original SMART on FHIR API is audacious and can be expressed concisely: an innovative app developer can write an app once and expect that it will run anywhere in the health care system. Further, that one app should be readily substitutable for another. When apps are substitutable, they compete with each other which drives up quality and down price. SMART supports an ‘App Store for Health’ model.”
It was bold. It was visionary. It was backed by industry, academia, and government leaders and funded by ONC with a $15M grant.
As FHIR gained momentum in the early 2010s, the natural convergence occurred around 2014. SMART on FHIR was born.
On paper, it was the perfect platform to restructure healthcare delivery through modular, substitutable apps.
Then it became even more significant.
In 2020, SMART on FHIR became a required standard supported by all certified EHRs.
The infrastructure was no longer optional. It was mandated.
A major acknowledgment goes to Kenneth Mandl and the entire SMART team for transforming an ambitious idea into the most widely adopted standard for open healthcare apps.
Fast Forward to 2025
We have the standards. We have the need. We have regulatory support, at least for now.
But do we have a genuine, thriving, app-based healthcare ecosystem?
In our view, not yet.
We are still operating in a world dominated by pilots, prototypes, connectathons, limited deployments, and impressive demos that do not scale into broad market adoption.
The “App Store for Health” vision has not fully materialized.
Why Hasn’t it Happened?
Darena Health was founded in 2009, alongside Meaningful Use and the launch of SMART. We have had a front-row seat through multiple cycles of optimism and recalibration.
From building a certified EHR, to working across several EHR ecosystems, to becoming the first company certified for G10, we have lived through the evolution of interoperability firsthand.
The reality is that technical standards alone do not create ecosystems.
An ecosystem requires:
True substitutability
Economic alignment
Clear distribution channels
Seamless integration into clinical workflows
Predictable monetization models
While SMART on FHIR created the rails, the market forces required to power an open, competitive app economy have been slower to align.
Why this Should Have Happened Already
The ingredients were there:
Standardized APIs
Mandated adoption
Developer tooling
Regulatory support
In theory, that should have unlocked innovation at scale.
In practice, variability in implementation, workflow friction, vendor incentives, and market fragmentation slowed the flywheel.
Healthcare is not consumer tech. Clinical workflows are complex. Risk tolerance is low. Procurement cycles are long.
But that does not mean the vision was flawed.
Why Now Might be Different
Several new forces are converging:
AI-native applications that require standardized data access
Increasing demand for modular, best-of-breed solutions
Financial pressure on health systems to improve efficiency
Emerging orchestration standards such as MCP that layer on top of FHIR
The conversation is shifting from “Can we access the data?” to “What can we build on top of it?”
We may finally be entering the phase where the infrastructure built over the last decade meets a technology wave capable of catalyzing real ecosystem growth.
The Bigger Question
The vision of an “App Store for Health” was never just about APIs. It was about competition, innovation, substitutability, and better outcomes.
The question is not whether SMART on FHIR worked. It clearly did, from a standards perspective.
The question is whether we are ready, culturally and economically, to unlock the ecosystem it was designed to enable.
We recently took a deeper dive into:
What the current app landscape actually looks like
Why this transformation should have happened already
Why it stalled
And why this moment might finally be different
We welcome perspectives from others who have been building in this space.
Has the healthcare app economy underperformed expectations? Or is it simply taking the natural pace of healthcare transformation?